What is Scoliosis?
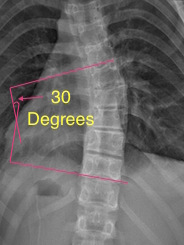
Figure 2
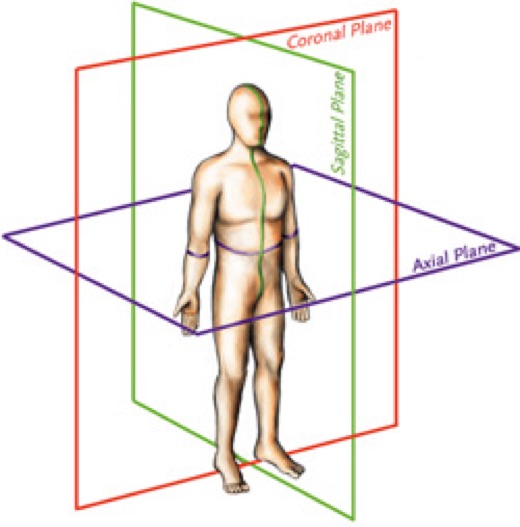
Figure 1
Scoliosis is a three dimensional medical condition in which the spine deviates in in all three planes of spinal motion (sagittal, coronal and axial).
Scoliosis can be congenital (caused by a spinal malformation at birth), idiopathic (cause which is unknown) and neuromuscular. Idiopathic represents approximately 80% of all cases of scoliosis, it is further classified as infantile, juvenile, adolescent and adult, which is based on when the onset occurred. Neuromuscular and congenital causes can be vast, and an extensive case history, neurological examination and radiology are required.
A scoliosis can present in an x-ray as a deviation that resembles an S or a C, rather than a straight line. The magnitude of this curve is then measured, which is referred to as a Cobb Angle – Figure 2.
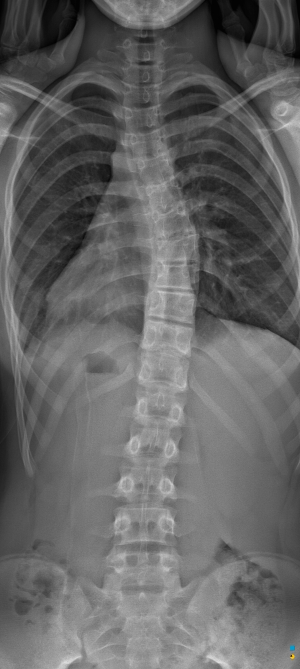
Figure 3

Figure 4
A spinal curvature with a Cobb Angle measurement greater than 10 degrees is considered a scoliosis, curvatures below 10 degrees are considered spinal asymmetries.
Figure 3 shows an example of a scoliosis curve. As the spine side-bends to one side, in the case of Figure 3 to the left, the spine will then consequently rotate to the right. This principal is one of Fryette’s laws. Fryette was an Osteopath who developed the principles of spinal mechanics in 1918, to classify dysfunctions in the axial skeleton. These principles are applied to the treatment of scoliosis.
A further test known as the Adam’s Forward Bending Test is used to measure the angle of trunk rotation, this measurement is related to the size of the Cobb Angle.1 Performing this test at regular intervals allows for ongoing monitoring of the curve in conjunction with x-rays.
Curve Classification
An x-ray of a scoliosis was traditionally reported as a C-Curve or an S-Curve. A C-Curve is also referred to as a 3 curve and an S-Curve is also referred to as a 4 curve. The scoliosis curve pattern in each individual is classified based on the number of curves present and the location of the curves within the spine. The Lehnert-Schroth augmented classification system (Figure 5) is used to prescribe Schroth Method exercises according to the individual’s curve pattern.
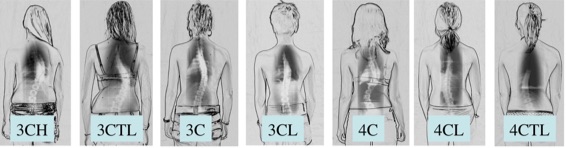
Figure 5: Lehnert-Schroth Augmented Classification
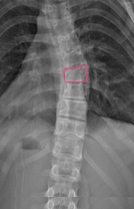
Figure 6
Each curve can either be structural or functional. Structural curves display as a change in the structure of the vertebrae at the apex of the curve.
Figure 6 shows how the vertebrae at the apex of the curve demonstrates some wedging. This is not present in the other vertebrae. The functional curves are the curves above and below the structural curve. They are only present to balance/level out the spine in an attempt to keep the head aligned over the centre of the pelvis.
It is this wedging of the vertebrae (structural change) that causes the asymmetrical loading of the spine and hence asymmetrical growth. It is unknown in idiopathic scoliosis why the initial wedging of the vertebrae occurs.
-
Read More About – Adolescent Idiopathic Scoliosis
Adolescent Idiopathic Scoliosis occurs in adolescents and has no known cause. This diagnosis is only formed when all other causes are excluded. It is the most common type of scoliosis representing approximately 80% of all cases. Females are approximately 4 times more likely to be affected by idiopathic scoliosis.1Approximately 2.5% of the population have a scoliosis, though only 0.25% progress to the point of requiring treatment (Bracing, Scoliosis Specific Exercise).2
Curves can progress rapidly during an adolescent’s growth period and then generally slow as the patient nears skeletal maturity. We are able to predict with some certainty the likelihood of the progression of a patients curve based on the age, skeletal maturity and current magnitude of curve.
There is a familial predisposition to idiopathic scoliosis, with 30% of patients reporting a family history.3 Studies have shown that when both parents have a scoliosis, their children have a 50 times increased risk of requiring treatment.4 Also if one child has a scoliosis the likelihood a sibling will have a curve ≥ 10 degrees is 19% and 11.5% ≥ 20 degrees.5
Adolescent patients rarely experience pain with a scoliosis, though visible asymmetries are normally present when looking from behind and are the first indicator a scoliosis may be present. Some of the possible asymmetries are listed below:
- Shoulder Height – one shoulder may sit higher than the other
- Shoulder Blade – one shoulder blade may sit higher than the other. Also the inside border may be more prominent
- Trunk Position – a shift of the trunk can be seen to one side
- Hip Prominence – one hip may be more prominent on one side. Appearing as though they are putting more weight onto that hip
- Head Position – the head may sit off to one side
- Rib Hump – this is a prominence of the ribs on one side. This is due to the rotation aspect of scoliosis (see Adam’s Forward Bending Test)
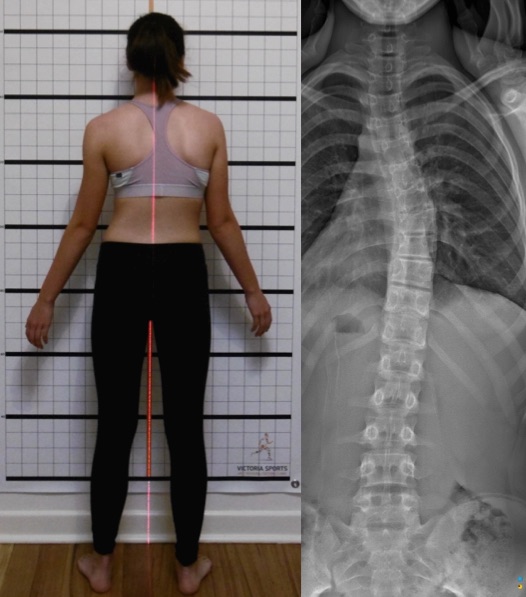
Figure 1: 3 Curve Posture

Figure 2: 4 Curve Posture
Figure 1: The above patient has a 3 curve – her trunk is seen translating to the right, her right shoulder blade is also more present, her left hip is more prominent and her head is slightly right of the midline.Figure 2: The above patient has a 4 curve – her trunk is seen translating to the left, her right shoulder is higher than her left, the lower border of her shoulder blade sits higher, her right hip is more prominent and her head is to the left of the midline.
1 – Weiss, HR, 2015. Schroth Therapy: Advancements in Conservative Scoliosis Treatment. 1st ed. Germany: Lambert.
2 – Asher M, Burton D. Adolescent idiopathic scoliosis: natural history and long term treatment effects. Scoliosis 2006, 1:2
3 – Scoliosis Research Scoiety. 2016. Adolescent Idiopathic Scoliosis. [ONLINE] Available at: http://www.srs.org/patients-and-families/conditions-and-treatments/parents/scoliosis/adolescent-idiopathic-scoliosis. [Accessed 04 January 16].
4 – Reamy B, Slakey J. Adolescent Idiopathic Scoliosis: Review and Current Concepts. Am Fam Physician. 2001 Jul 1
5 – Wise C, Gao X, Shoemaker S, Gordon D, Herring J. Understanding Genetic Factors in Idiopathic Scoliosis, a Complex Disease of Childhood. Curr Genomics. 2008 Mar -
Read More About – Adult Degenerative Scoliosis
 Scoliosis in adults is due to degeneration of the disc and facet joints of the spine. This can start to occur later in life or may be due to an existing adolescent scoliosis. Due to the uneven loading of the bones of the spine, it causes asymmetrical growth and degeneration leading to further progression of the curve. Pain symptoms are commonly associated with Adult Degenerative Scoliosis.
Scoliosis in adults is due to degeneration of the disc and facet joints of the spine. This can start to occur later in life or may be due to an existing adolescent scoliosis. Due to the uneven loading of the bones of the spine, it causes asymmetrical growth and degeneration leading to further progression of the curve. Pain symptoms are commonly associated with Adult Degenerative Scoliosis.Treatment using the Schroth Method aims to stabilise the spine through strengthening the spinal muscles, improving spinal mobility and improving posture in the areas contributing to the pain and progression of the curvature.
While chronic pain as a result of a scoliosis can occur with any degree of curve, the larger the curve the larger the incidence of chronic pain.1 Approximately 61% of adults with a scoliosis will experience chronic pain.2 So if we can reduce the progression of the curve, we can hopefully reduce the amount of pain experienced that can affect a patients quality of life.
1 – Kostuik JP, Bentivoglio J. The incidence of low-back pain in adult scoliosis. Spine (Phila Pa 1976). 1981 May-Jun
2 – Weinstein SL, Dolan LA, Spratt KF, Peterson KK, Spoonamore MJ, Ponseti IV. Health and function of patients with untreated idiopathic scoliosis: a 50-year natural history study. JAMA. 2003 Feb
1 – Samuelsson L, Norén L. Trunk rotation in scoliosis. The influence of curve type and direction in 150 children. Acta Orthop Scand. 1997 Jun
2 – Negrini S, Donzelli S, Lusini M, Minnella S, Zaina F. The effectiveness of combined bracing and exercise in adolescent idiopathic scoliosis based on SRS and SOSORT criteria: a prospective study. BMC Musculoskelet Disord. 2014.
3 – Kuroki H, Inomata N, Hamanaka H, Higa K, Chosa E, Tajima N. Predictive factors of Osaka Medical College (OMC) brace treatment in patients with adolescent idiopathic scoliosis. Scoliosis 2015